Menopause-related urinary incontinence reflects estrogen decline affecting the urethra, bladder lining, and pelvic floor.
Estrogen maintains collagen strength, vascular support, and urethral closure pressure. Loss of hormonal support leads to thinner tissues and increased bladder reactivity, contributing to stress, urge, or mixed incontinence.
Doctors assess symptom type and severity, GSM features, age, time since menopause, cardiometabolic and risk profile, medical history, and coexisting conditions.
Management may include local vaginal estrogen, systemic hormone therapy, pelvic floor rehabilitation, or bladder-specific medications.
Treatment response varies based on underlying mechanism and tissue health.
Care involves appropriate evaluation and follow-up to monitor safety, symptom change, and functional improvement over time.
Menopause and Urinary Incontinence: Causes and Reclaiming Control
 Hailey Kean
Hailey Kean Dr. Saranne Perman, MD
Dr. Saranne Perman, MDThe Bottom Line:
Bladder leakage during perimenopause and menopause is far more common than many realize. Studies show that 38%–55% of women over age 60 experience urinary incontinence (UI).(1)
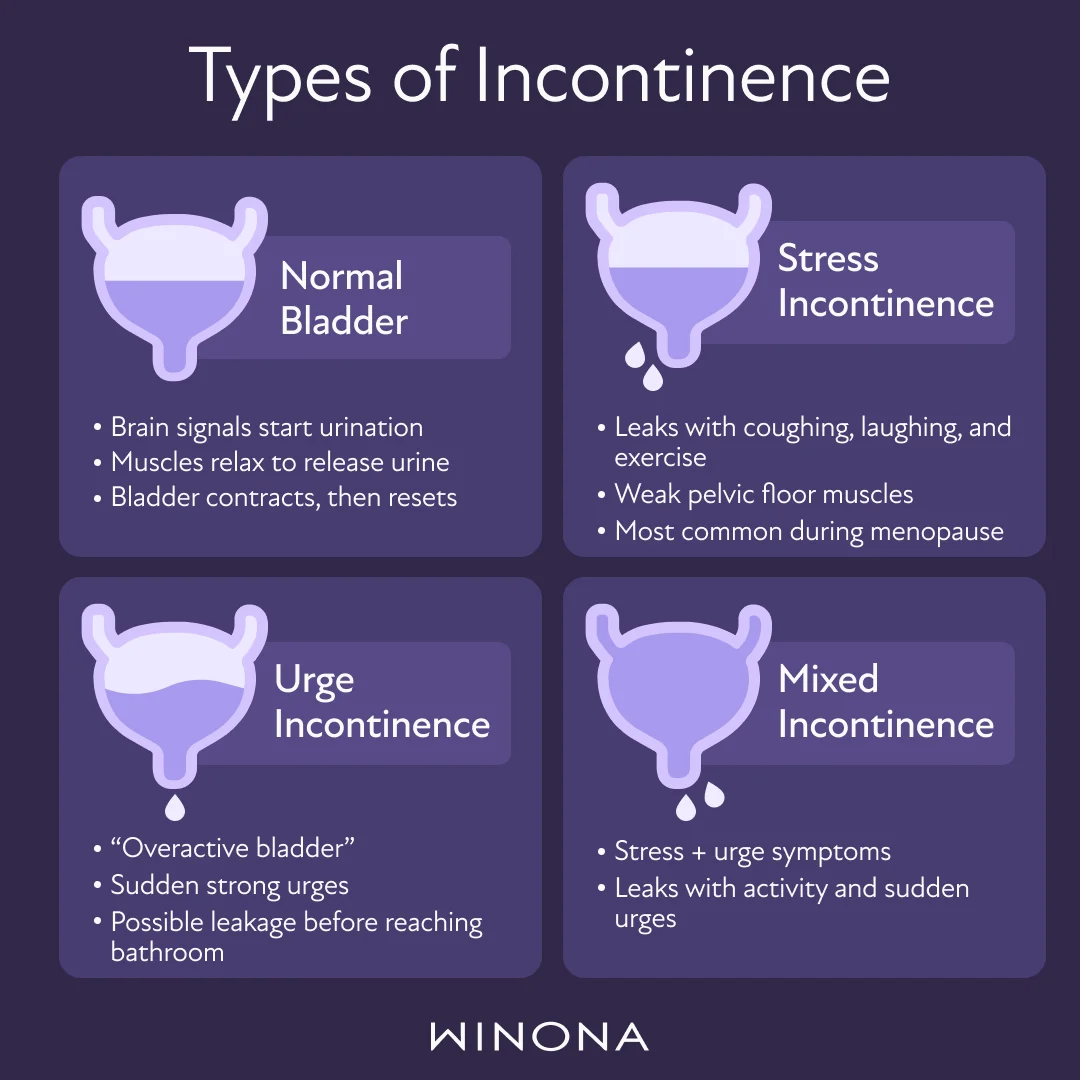
Symptoms may involve small leaks caused by activities such as coughing or sneezing (stress incontinence) or a sudden need to urinate that’s hard to delay (urge incontinence). These changes often stem from shifting hormone levels, weakening pelvic floor muscles, and changes in the urethra and vagina that make bladder control harder to maintain.(2)(3)
Urinary incontinence also falls under the genitourinary syndrome of menopause (GSM), a broader collection of symptoms that includes vaginal dryness, irritation, and discomfort during intercourse. Recognizing urinary leakage as part of GSM can help explain why bladder symptoms often occur alongside sexual discomfort and other pelvic changes.(2)(4)
Menopause can also influence the bladder muscles and the nerves that coordinate urination. Together, these changes can lead to stress incontinence, urge incontinence, or a mix of both.
This article explains why bladder control changes happen, how estrogen affects pelvic tissues, and the full range of treatment options — from pelvic floor muscle training to hormone therapy, vaginal devices, and surgical procedures — that can provide meaningful improvement.
Why Menopause Affects Bladder Control: The Physiological Causes
Low estrogen affects nearly every structure involved in bladder control. The pelvic floor muscles lose strength, the urethra loses support, and the tissues of the lower urinary tract become thinner and less elastic. These changes fall under GSM, a well-established collection of symptoms that includes dryness, discomfort, recurrent UTIs, and urinary incontinence.(1)(2)
The Role of Estrogen in Pelvic Health
Estrogen plays a central role in maintaining the health of the pelvic organs. It helps keep collagen strong, supports blood flow, and maintains the thickness and elasticity of tissues in the urethra, bladder, and vagina. When estrogen levels fall during perimenopause and menopause, several changes follow:(1)(2)(3)
The urethra loses its tight seal, making leaks more likely during movement or activity.
Bladder muscles become more reactive, contributing to an overactive bladder.
The pelvic floor has less hormonal support, which can reduce its strength.
Research in urogynecology repeatedly shows that lower estrogen levels are linked to higher rates of urgency, frequency, and leakage. Restoring estrogen directly to the vaginal and urethral tissues can improve these symptoms by rebuilding tone and moisture.(1)(3)
Weakening of the Pelvic Floor Muscles
The pelvic floor is a group of muscles that supports the bladder, uterus, and bowel. These muscles contract and relax to maintain control over urination. During menopause, several factors can weaken this system:(1)(2)(3)
Aging and reduced collagen
Increased abdominal pressure from weight gain or chronic coughing
Past childbirth injuries
Reduced estrogen support
When the pelvic floor cannot tighten effectively, activities like coughing, laughing, exercising, or lifting can trigger stress incontinence.
Thinning of Urethral and Vaginal Tissues (GSM)
GSM causes noticeable changes in the vagina, urethra, and surrounding tissues. Without adequate estrogen, these tissues become drier, thinner, and less elastic.(4)
This leads to the following:
Increased friction and irritation
Greater susceptibility to urinary tract infections
Reduced support for the urethra
Heightened urgency and frequency
These changes help explain why urge incontinence and overactive bladder often worsen during menopause.
Risk Factors That May Worsen Incontinence During Menopause
Several factors can increase the likelihood of developing urinary incontinence during menopause or intensify existing symptoms. Key contributors include the following:(1)(2)(3)(4)
Lifestyle Factors: Sedentary habits, like prolonged sitting at work, frequent car use, or lack of physical activity, can weaken overall muscle function, including the pelvic floor.
Genetic Predisposition: A higher incidence of UI is observed in women with a family history of urinary incontinence, suggesting a genetic factor in its development.
Pregnancy and Childbirth: The number of pregnancies and the nature of childbirth influence UI risk. Cesarean deliveries may lower the risk, whereas higher birth weights (more than eight pounds) and multiple natural births may increase it.
Obesity: Abdominal obesity significantly raises the risk of UI. Medical studies indicate that obese women are 4–5 times more likely to suffer from incontinence.
Health Conditions: Several medical issues can increase UI risk, including urinary tract infections, chronic constipation, diabetic neuropathy, neurological disorders like Parkinson’s disease and multiple sclerosis, and chronic respiratory diseases like COPD, which increase abdominal pressure and potentially worsen UI.
Medications: Certain drugs, including diuretics, antihypertensives, and anxiolytics (medicines to manage anxiety symptoms), may influence the occurrence of UI by affecting bladder control or muscle strength.
Recognizing these risk factors can help guide both prevention and treatment strategies.
Diagnosing Urinary Incontinence
A thorough evaluation helps identify the type and cause of urinary incontinence. Board-certified physicians trained in menopause typically begin with a medical history, physical examination, and vaginal exam. They may also measure post-void residual volume — the amount of urine left after urinating — and check for conditions that can mimic urinary incontinence, like a urinary tract infection.(1)
A Comprehensive Plan for Managing Incontinence
The Menopause Society notes that bladder and urinary tract concerns are frequently ignored or minimized during the menopause transition. The good news is that menopause-related urinary incontinence can be improved through a combination of behavioral strategies, targeted exercises, medications, estrogen therapy, and, in more severe cases, surgeries.(5)
The most effective plans use several approaches together.
The Foundation: Pelvic Floor Exercises (Kegels)
Kegel exercises strengthen the pelvic floor muscles that control the urethra and support the bladder. Stronger muscles can reduce stress incontinence and improve bladder stability.(6)
How to Find the Right Muscles
The easiest way is to imagine stopping a leak of urine or holding in gas. Those muscles should tighten and lift. Once identified, practice them when the bladder is empty.
How to Perform Kegels
Tighten the pelvic floor as if preventing a leak
Hold for 3–5 seconds
Relax for 3–5 seconds
Repeat 10 times
Aim for three sessions a day
Kegels can be done while sitting, lying down, or standing. With consistent practice, many notice fewer leaks and stronger bladder control.
Behavioral Techniques: Bladder Training and Lifestyle Habits
Bladder training teaches the bladder to wait longer between trips to the bathroom. This improves urgency, reduces frequency, and supports the bladder muscles.
Bladder training involves three key steps:(1)(2)
Note current bathroom frequency
Add 5–10 minutes between restroom visits
Gradually increase intervals over several weeks
Lifestyle habits that support bladder control include the following:(1)(2)(3)
Limiting caffeine and alcohol, which can irritate the bladder
Maintaining regular bowel movements to reduce constipation
Managing weight — even modest weight loss can improve symptoms
Avoiding high-impact activities that strain the pelvic floor
Planning regular bathroom breaks throughout the day
Practicing double voiding to ensure the bladder empties fully
These combined strategies help improve comfort and strengthen bladder function.

Medical Treatments to Restore Tissue Health
Vaginal Estrogen
Vaginal estrogen, or localized hormone therapy, is one of the most effective treatments for menopause-related urinary symptoms. Delivered as creams, gels, or inserts, it helps rebuild the tissues of the vagina and urethra without significant systemic absorption.(1)(4)
Benefits include the following:
Improved moisture and elasticity
A stronger urethral seal
Fewer UTIs
Reduced urgency and frequency
Systemic HRT
Systemic hormone replacement therapy — delivered through patches, creams, or pills — may support urinary and pelvic health when used alongside other treatments. Although not prescribed solely for bladder control, it can help reduce urgency and overactive bladder symptoms.(2)(4)
Medications for Bladder Muscles
Medications may calm bladder muscles or increase bladder capacity. Common options include the following:(1)
Anticholinergics
Beta-3 adrenergic agonists
These medications are often used when lifestyle changes are not enough.
Additional Hormonal Support: DHEA
DHEA, used in low doses, converts into estrogen and testosterone. It may help improve vaginal and urethral tissue health, as well as support pelvic muscle function.(4)
Vaginal Devices for Structural Support
Vaginal support devices may also help reduce leakage, especially stress incontinence:(2)
Pessaries support the urethra and bladder neck
Urethral inserts may help prevent leakage during specific activities
These devices are typically fitted or prescribed by a doctor.
Surgeries for Severe Cases
When conservative treatments are not successful, surgical procedures may be used to reposition or support the bladder and urethra. These surgeries target stress incontinence and are considered only after other approaches have been explored.(1)(2)
Moving Forward with Confidence
Menopause can bring new changes to bladder control, but these symptoms are treatable. Understanding how estrogen, pelvic floor muscles, and the urethra shift during this stage can guide an effective treatment plan. Early management often leads to better comfort, stronger bladder control, and greater confidence in daily routines.
Experiencing menopausal urinary incontinence? Discover if HRT is right for you.
Take Winona's brief menopause quiz to see whether our treatment options may help support your bladder health and improve symptoms.
Frequently Asked Questions (FAQs) About Incontinence in Menopause
Low estrogen can contribute to urinary leakage during the menopause transition. Estrogen supports the strength and elasticity of the tissues that line the urethra and helps maintain healthy pelvic floor muscles. When estrogen declines, these tissues can thin and lose firmness, which can reduce bladder support.
This change can increase the likelihood of stress incontinence or sudden urges to urinate. Other factors like childbirth history, weight, and certain medical conditions can add to these symptoms, but reduced estrogen plays a central role.
Bladder changes can begin in perimenopause. Hormone levels shift during this stage, and these fluctuations can affect the tissues that support bladder control. Many individuals first notice mild leakage or increased urgency during perimenopause, sometimes years before their final menstrual period. These early symptoms often reflect the gradual decline in estrogen and shifts in pelvic floor strength. Recognizing these signs early can help guide steps to support bladder health throughout the transition.
Managing bladder leakage after menopause often requires a tailored approach. Strengthening the pelvic floor with Kegel exercises can improve support for the bladder and urethra. Daily habits — like spacing fluids throughout the day, choosing bladder-friendly beverages, and maintaining regular bowel movements — may also help.
Medical treatment is another option. Vaginal estrogen can support tissue health in the urethra and vagina, which may ease symptoms. In some cases, other therapies or devices may be recommended by a physician based on the type of incontinence and its severity.
Hydration plays an important role in bladder comfort. Drinking too little water can make urine more concentrated, which may irritate the bladder and worsen urgency or discomfort. Most people do well with six to eight glasses of fluid daily, unless a physician recommends otherwise. Spacing fluids evenly throughout the day can support bladder function. Some individuals prefer to reduce fluid intake close to bedtime to limit nighttime trips to the bathroom.
Research suggests that vitamin D may support pelvic floor muscle function, which could help reduce the frequency or severity of certain incontinence symptoms. Still, no vitamin serves as a direct treatment for bladder leakage. Pelvic floor strengthening, lifestyle adjustments, and medical therapies remain the most effective approaches. A physician can best determine whether vitamin D or other supplements are appropriate within a person’s overall health plan.
This article is for informational purposes only and does not constitute medical advice. The information contained herein is not a substitute for professional medical advice. Always talk to your doctor about the risks and benefits of any treatment.